
Acknowledgements: Jan Hooper, Director of Nursing (medical), kindly allowed us to take photographs of the now outdated PhotoCure ASA machine. Dr Warren Weightman, head of the Dermatology Department at TQEH, provided the information and a photograph of a current model.
The concept of Photodynamic Therapy has been known for a long time.At the beginning of the 20th century Niels Finsen and Oscar Raab noted that haemato-porphyrin had a tumour-localising tendency. They also noted that if the tumour was then irradiated with a red light ( >610 nm) it produced a photo-toxic effect on the tumour cells. In the last 25 years this method of treatment became more popular and is now expanding into all fields of medicine and surgery.
The literature reports by the proponents of this method of treatment claim a success rate similar to cryotherapy and surgery when used in the treatment of hyperkeratoses, basal cell skin cancers and other suitable lesions.
In South Australia early 1990s Dr. Ian Forbes then a Reader in Medicine at the Queen Elizabeth Hospital in Adelaide.used intravenous injection of a heamato-porphyrin derivative (HpD). It was preferentially concentrated in skin lesions and after irradiation with a red light source with a wavelength of 620 nanometers (nm) he achieved several cures. In one instance he treated local recurrences (small nodules) after mastectomy and achieved a cure.(personal communication Michal Patkin). The associated transient photosensitivity however was troublesome.
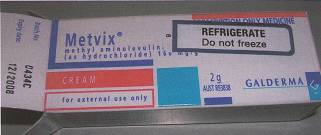
The QEH Dermatology Department later purchased a PhotoCure ASA machine from Norway for the same reason. In addition the company also supplied a cream Metvix which when applied directly to the lesion confined the photo-sensitivity to the local area only. It was used with success in selected cases and when the company produced a new more efficient model the old machine was replaced.
More recently the combination of photo-sensitising agent and illumination is also used for diagnostic purposes. An agent Hexvix is injected intravenously. Because it is preferentially concentrated in a polyp or tumour. It fluoresces if illuminated with appropriate light source. It is claimed that this type of imaging improves the accuracy of diagnosis in bladder, colon or bronchial tumours and has treatment possibilities.

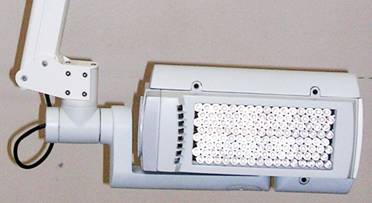
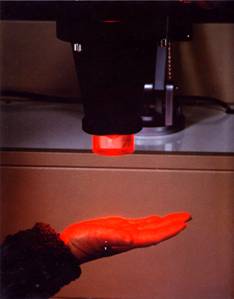
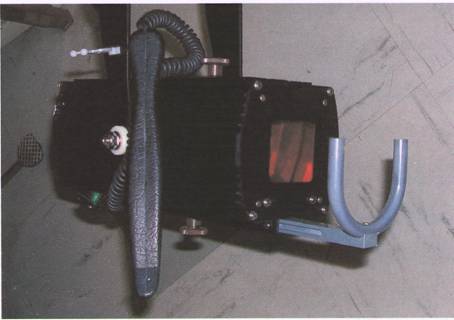 Light source, usually > 610 nm with switch and adjustable distance probe
Light source, usually > 610 nm with switch and adjustable distance probe
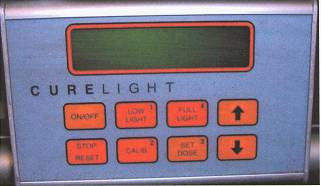
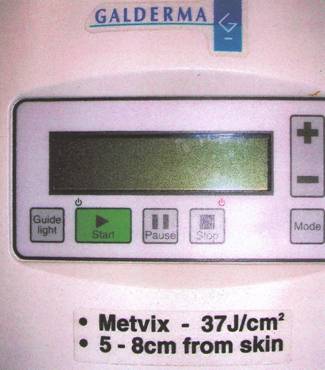
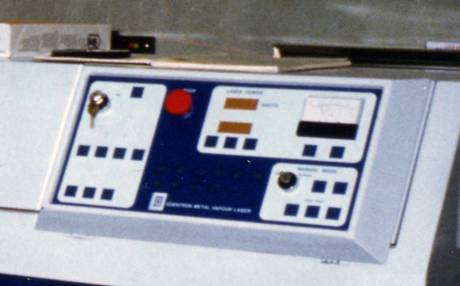
Control panel of the machine

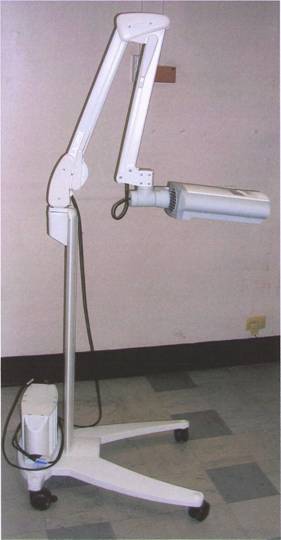
Photodynamic machine currently used at TQEH. Supplied by an Australian branch of the Swiss company Galderma
Light source
Control panel


Photodynamatic machine currently used at the QEH



Addendum
Acknowledgment: The following photographs have been provided by Dr. Prue Cowled, Principal Scientist in the Department of Surgery at The Queen Elizabeth Hospital, Adelaide. The details and information has been kindly supplied by Dr. Ian Forbes.
The haemato-porpyrin was prepared in the University Department of Chemistry and the Pharmacy Department of the Hospital provided the required sterile conditions.
The light source was made in the Physics Department of the University of Adelaide. Later, a gold laser was used. This provided a red light at 627.8 nm and was developed by Quentron Optics, a South Australian company.
In some instances the results were spectacular but the therapy had little effect on advanced or large tumours. In addition several treatments and occasional anaesthetics were needed and the photosensitivity that followed was troublesome.

The incandescent light source 620-640 nm. Built by the physics department, the red lamp is top left.
Close up view of the lamp

 Fibro-optic cable passed through a bronchoscope
Fibro-optic cable passed through a bronchoscope

Under general anaesthetic. Fibro-optic cable is passed through the biopsy channel of the bronchoscope to illuminate the tumour. Bronchoscope held by clamp
.

An attempt to treat a brain tumour during a craniotomy.


Needles inserted into a recurrent skin nodule following mastectomy with a successful result.
(The patient had been operated on earlier by Michael Patkin, webmaster of this site, to whom the outcome of phototherapy appeared extraordinary).

-o0o-